 |
Toll Free 877-238-1437
|
Prostate Cancer Publications
Prostate Publications and Articles
- High-dose-rate intensity modulated brachytherapy with External Beam Irradiation for Prostate Cancer: California endocurietherapy's 10-year results
- Lack of Benefit from A Short Course of Androgen Deprivation for Unfavorable Prostate Cancer Patients Treated with an Accelerated Hypofractionated Regime
- High Dose Rate Monotherapy for Prostate Cancer Early Result
- Lack of Benefit of Pelvic Radiation in Prostate Cancer Patients with a High Risk of Positive Pelvic Lymph Nodes Treated with High-Dose Radiation
- High Dose Rate Monotherapy for Prostate Cancer: CET's 5-year results
- Long Term Results of HDR Brachytherapy and external Beam with and without short term androgen suppression for prostate cancer
- High dose rate prostate brachytherapy: the California Endocurietherapy (CET) Method
- How to compare published prostate study results
Back to Top 1. High-dose-rate intensity modulated brachytherapy with External Beam Irradiation for Prostate Cancer: California endocurietherapy's 10-year results
Article Name: High-dose-ate intensity modulated brachytherapy with External Beam Irradiation for Prostate Cancer: California endocurietherapy's 10-year results.Author: D. Jeffrey Demanes, M.D.,
Published Date: April 2005
Medical Journal: International Journal of Radiation Oncology Biology and Physics (IJROBP), Vol. 61, No.5, 99 1306-1316, 1 April 2005.
Abstract
Purpose:To present the long-term outcome and morbidity of high-dose-rate brachytherapy (HDR-BT) combined with external beam radiotherapy (EBRT) for localized prostate cancer. |
Methods and Materials:Between September 1991 and December 1998, 209 consecutive patients with no prior androgen suppression were treated with HDR-BT plus EBRT. The median follow-up was 7.25 years (range, 5–12 years). The patients were stratified into three risk groups: low (Stage T2a or less, Gleason score ≤6, and prostate-specific antigen [PSA] level ≤10 ng/mL), intermediate (Stage T2b,c, Gleason score 7, and PSA level 10–20 ng/mL), and high (Stage T3, Gleason score 8–10, and PSA level >20). Four definitions of PSA progression were compared with the general clinical failure outcome: the American Society for Therapeutic Radiology and Oncology (ASTRO) definition, nadir plus 2.0 ng/mL, two consecutive rises ≥0.5 ng/mL, and PSA level >0.2 ng/mL. Morbidity was scored using Radiation Therapy Oncology Group criteria. |
Results:The general clinical control rate was 90% (188 of 209), and the general clinical failure rate was 10% (21 of 209). The overall survival rate was 79%, and the cause-specific survival rate was 97%. The PSA progression-free survival (ASTRO definition) rate was 90%, 87%, and 69% for the low-, intermediate-, and high-risk groups, respectively. The nadir plus 2 ng/mL and two rises ≥0.5 definitions correlated better with the actual clinical outcome than did the ASTRO and PSA >0.2 ng/mL definitions. The rate of Grade 3 and 4 late urinary morbidity was 6.7% and 1%, respectively, mostly occurring in patients who had undergone post-RT transurethral prostate resection. No late Grade 3 or 4 rectal morbidity developed. The sexual potency preservation rate was 67%. |
Conclusion:Our 10-year results have demonstrated HDR-BT plus EBRT is a proven treatment for all stages of localized prostate cancer. The morbidity was low, but post-RT transurethral resection should be avoided. |
Back to Top 2. Lack of Benefit from A Short Course of Androgen Deprivation for Unfavorable Prostate Cancer Patients Treated with an Accelerated Hypofractionated Regime
Article Name: High Dose Rate Intensity Modulated Brachytherapy with External Beam Irradiation for Prostate CancerAuthor: Alvaro A. Martinez, M.D., F.A.C.R.,* D. Jeffrey Demanes, M.D.,† Razvan Galalae, M.D.,‡ Carlos Vargas, M.D.,* Hagen Bertermann, M.D.,‡
*Departments of Radiation Oncology and Urology, William Beaumont Hospital, Royal Oak, MI; †California Endocurietherapy Cancer Center, Oakland, CA; and ‡Departments of Radiation Oncology and Urology, Kiel University Hospital, Kiel, Germany
Published Date: April 2005
Medical Journal: International Journal of Radiation Oncology Biology and Physics (IJROBP), Vol. 61, No.5, 99 1306-1316, 1 April 2005.
Abstract
Purpose:High-dose radiotherapy, delivered in an accelerated hypofractionated course, was utilized to treat prostate cancer. Therapy consisted of external beam radiotherapy (EBRT) and transrectal ultrasound (TRUS)-guided conformally modulated high-dose rate (HDR) brachytherapy. The purpose of this report is (1) to assess long-term comparative outcomes from three trials using similar accelerated hypofractionated regimes; and (2) to examine the long-term survival impact of a short course of £ 6 months adjuvant/ concurrent androgen deprivation when a very high radiation dose was delivered. |
Methods and Materials:Between 1986 and 2000, 1,260 patients were treated at three institutions with pelvic EBRT (36 –50 Gy) integrated with HDR prostate brachytherapy. The total dose including brachytherapy was given over 5 weeks. The biologic equivalent EBRT dose ranged between 90 and 123 Gy (median, 102 Gy) using an a /b of 1.2. Patient eligibility criteria included a pretreatment prostate-specific antigen ³10, Gleason score ³7, or clinical stage ³T2b. A total of 1,260 patients were treated, and 934 meet the criteria. Kiel University Hospital treated 198 patients; William Beaumont Hospital, 315; and California Endocurietherapy Cancer Center, 459 patients. Brachytherapy dose regimes were somewhat different between centers and the dose was escalated from 5.5 x 3 to 15 Gy x 2 Gy. Patients were divided for analysis between the 406 who received up to 6 months of androgen deprivation therapy and the 528 patients who did not. All patients had a minimum follow-up of 18 months (3 times the exposure to androgen deprivation therapy). The American Society for Therapeutic Radiology and Oncology biochemical failure definition was used. |
Results:Mean age was 69 years. Median follow-up time was 4.4 years (range, 1.5–14.5); 4 years for androgen deprivation therapy patients and 4.9 for radiation alone. There was no difference at 5 and 8 years in overall survival, cause-specific survival, or biochemical control among the three institutions. The corresponding 8-year rates with and without androgen deprivation therapy were biochemical control 85% and 81%; overall survival 83% and 78%; cause-specific survival 89% and 94%; and metastatic rates of 16.6% and 7.3%. A multivariate analysis revealed androgen deprivation therapy did not predict for biochemical failure for either the entire group or the subset of 177 patients harboring all three poor prognostic factors. Moreover, adding androgen deprivation therapy strongly correlated with higher rates of both metastasis (r = 0.09; hazard ratio, 2.08) and cancer-related deaths (r = 0.02, hazard ratio 3.25). These negative results for the most unfavorable group led us to question if androgen deprivation therapy might have a deleterious impact through delay in delivery of the potentially curative radiation or whether there may be a biologic basis by fixing the cycling cells in G0. |
Conclusion:Accelerated hypofractionated pelvic EBRT integrated with TRUS-guided conformally modulated HDR administered to 1,260 patients in three institutions was an excellent method of delivering very high radiation dose to the prostate in 5 weeks. Similar high overall, cause-specific, and biochemical no evidence of disease survival rates achieved show that prostate HDR can be successfully delivered in academic and community settings. At 8 years, the addition of a course of £6 months of neoadjuvant/concurrent androgen deprivation therapy to a very high radiation dose did not confer a therapeutic advantage but added side effects and cost. Furthermore, for the most unfavorable group, there was a higher rate of distant metastasis and more prostate cancer–related deaths. We question the value of a short course of androgen deprivation therapy when used with high-dose radiation. |
Back to Top3. High Dose Rate Monotherapy for Prostate Cancer Early Result
Author: D. Jeffrey Demanes, M.D., Gillian Altieri, C.M.D. David Brandt, M.A. ,Lionel Schour, M.D., Marie-Claire Barnaba, M.S.N.-N.P., Pat Skoolisariyaporn M.S.
Presented Date: Presentation at American Society for Therapeutic Radiology and Oncology (ASTRO) Conference October 2005
| Links to Poster: | 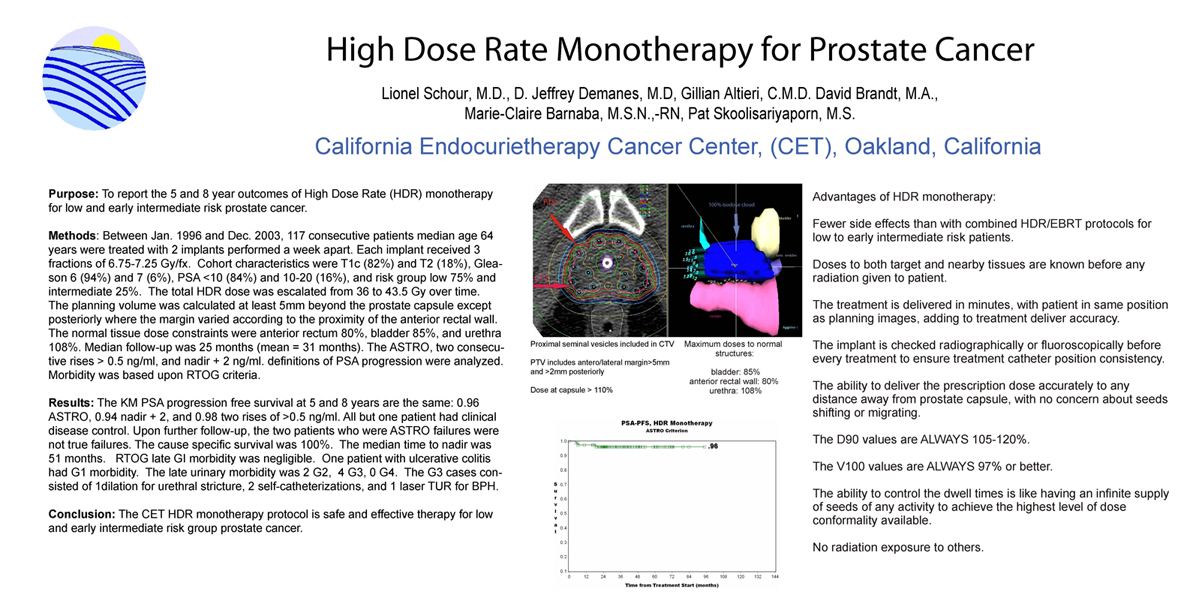 |
 |
Abstract:
Purpose:To report the 5 and 8 year outcomes of High Dose Rate (HDR) monotherapy for low and early intermediate risk prostate cancer. |
Methods and Materials:Between Jan. 1996 and Dec. 2003, 117 consecutive patients median age 64 years were treated with 6 HDR fractions delivered in 2 procedures 1 week apart. Disease characteristics were T1c (82%) or T2 (18%), Gleason 6 (94%) and 7 (6%), PSA < 10 (84%) and 10-20 (16%), and risk group low 75% and intermediate 25%. The dose was escalated from 36 to 43.5 Gy over time. The planning volume was calculated 5mm beyond the prostate capsule. The normal tissue dose constraints were anterior rectum 80%, bladder 85%, and urethra 108%. Median follow-up was 25 months (mean = 31 months). The ASTRO, two consecutive rises ³ 0.5 ng/ml, and nadir + 2 ng/ml. definitions of PSA progression were analyzed. Morbidity was based upon RTOG criteria. |
Results:The KM PSA progression free survival at 5 and 8 years are the same: 0.96 ASTRO, 0.94 nadir + 2, and 0.98 two rises of ³ 0.5 ng/ml. All but one patient has clinical disease control. Only two patients had PSA progression according to the ASTRO definition of failure which with further follow-up, were false positives . The cause specific survival is 100%. The median time to nadir is 51 months. RTOG late GI morbidity was negligible. One patient with ulcerative colitis had G1 morbidity. The late urinary morbidity was 2 G2, and 4 G3, 0 G4. The G3 cases consisted of 1dilation for urethral stricture, 2 self-catheterizations, and 1 laser TUR for BPH. |
Conclusion:The CET HDR monotherapy protocol is safe and effective therapy for low and early intermediate risk group prostate cancer. |
Back to Top4. Lack of Benefit of Pelvic Radiation in Prostate Cancer Patients with a High Risk of Positive Pelvic Lymph Nodes Treated with High-Dose Radiation
Article Name: High Dose Rate Intensity Modulated Brachytherapy with External Beam Irradiation for Prostate CancerAuthor: Carlos Enrique Vargas, M.D.,* Razavan Galalae, M.D.,† Jeffery Demanes, M.D.,‡ Asif Harsolia, M.D.,* Elisa Meldolesi, M.D.,* Nils Nürnberg, M.D.,§ Lionel Schour, M.D.,‡ and Aalvaro Martinez, M.D.*
Published Date: April 2005
Medical Journal: International Journal of Radiation Oncology Biology and Physics (IJROBP), Vol. 61, No.5, 99 1306-1316, 1 April 2005.
Abstract
Purpose:The use of pelvic radiation for patients with a high risk of lymph node (LN) metastasis (>15%) remains controversial. We reviewed the data at three institutions treating patients with a combination of external-beam radiation therapy and high-dose-rate brachytherapy to address the prognostic implications of the use of the Roach formula and the benefit of pelvic treatment. |
Methods and Materials:From 1986 to 2003, 1,491 patients were treated with external-beam radiation therapy and high-dose-rate brachytherapy. The Roach formula [2/3 prostate-specific antigen + (Gleason score -6) x 10] could be calculated for 1,357 patients. Group I consisted of patients having a risk of positive LN £15% (n = 761), Group II had a risk >15% and £30% (n = 422), and Group III had a risk of LN disease >30% (n = 174). A >15% risk of having positive LN was found in 596 patients and was used to determine the benefit of pelvic radiation. The pelvis was treated at two of the cancer centers (n = 312), whereas at the third center (n = 284) radiation therapy was delivered to the prostate and seminal vesicles alone. Average biologic effective dose was >100 Gy (ab 1.2). Biochemical failure was as per the American Society for Therapeutic Radiology and Oncology definition. Statistics included the log–rank test as well as Cox univariate and multivariate analysis. |
Results:For all 596 patients with a positive LN risk >15%, median follow-up was 4.3 years, with a mean of 4.8 years. For all cases, median follow-up was 4 years and mean follow-up was 4.4 years. Five-year results for the three groups based on their risk of positive LN were significantly different in terms of biochemical failure (r < 0.001), clinical control (r < 0.001), disease-free survival excluding biochemical failure (r < 0.001), cause-specific survival (r < 0.001), and overall survival (r < 0.001). For all patients with a risk of positive LN >15% (n = 596), Group II (>15–30% risk), or Group III (>30% risk), no benefit was seen in the 5-year rates of clinical failure, cause-specific survival, or overall survival with pelvic radiation. In the Cox multivariate analysis for cause specific survival, Gleason score (r = 0.009, hazard ratio [HR] 3.1), T stage (r = 0.03, HR 1.8), and year of treatment (r = 0.05, HR 1.1) were significant. A log–rank test for cause-specific survival for all patients (n = 577) by the use of pelvic radiation was not significant (r = 0.99) accounting for high-dose-rate brachytherapy dose, |
Conclusion:The use of the Roach formula to stratify patients for clinical and biochemical outcomes is excellent. Pelvic radiation added to high prostate radiation doses did not show a clinical benefit for patients at a high risk of pelvic LN disease (>15%) selected using the Roach formula. |
Back to Top5. High-dose-rate monotherapy for prostate cancer: CET's 5-year results
Article Name: High Dose Rate Intensity Modulated Brachytherapy with External Beam Irradiation for Prostate CancerAuthor: D Jeffrey Demanes, M.D. , Gillian Altieri, C.M.D. , David Brandt, M.A., Marie-Claire Barnaba, M.S.N.-N.P., Lionel Schour, M.D., Pat Skoolisariyaporn, M.S. California Endocurietherapy Cancer Center, Oakland, CA
Published Date: Presentation at American Brachytherapy Society (ABS) Conference April 20005
Medical Journal:
Abstract
Purpose:To report the outcome of high-dose-rate brachytherapy as monotherapy for prostate cancer. |
Methods and Materials:Between Jan. 1996 and Dec. 2002, 80 consecutive patients were treated with HDR monotherapy. Patients were selected for monotherapy if they had low or early intermediate risk factors. The protocol was 6 HDR fractions (6.75-7.0 Gy). Disease characteristics were T1c (85%) or T2 (15%), Gleason 6 (97%) and 7 (3%), PSA < 10 (83%) and 10.20 (17%), and risk groups low 79% and intermediate (21%). The planning volume was calculated at least 5mm beyond the prostate capsule. The normal tissuedose constraints were rectum 75%, bladder 80%, and urethra 110%. Median follow-up was 3 years. the ASTRO definition of PSA progression was used. Morbidity was scored using TROG criteria. |
Results:The KM 5 year PSA progression control rate was 96%. All but one patient had PSA and clinical disease control. Local regional control was 99%. Cause specific survival was 100%. he median time to nadir was 28 months. Acute radiation morbidity resolved within 1 month. RTOG late gasto-intestinal morbidity was minimal. One patient with ulcerative colitis had G1 morbidity. Late genito-unrinary morbidity was 5 G1 (6.3%), 2 G2 (2.5%), 3 G3 (3.75%), and 0 G4. the G3 cases consisted of 1 urethral stricture dilation, 1 self-catheterization, and 1 laser TUR for BPH. The dosimetry was highly conformal. The D90 range was 105% - 115% of the prescription dose. |
Conclusion:The CET HDR monotherapy protocol is an effective treatment for low and early intermediate risk prostate cancer. Dosimetry was consistently good and prospectively assured accurate dose delivery. the late morbidity rate is low. |
Back to Top6. Long Term Results of HDR Brachytherapy and external Beam with and without short term androgen suppression for prostate cancer
Article Name:Long Term Results of HDR Brachytherapy and external Beam with and without short term androgen suppression for prostate cancerAuthor: D Jeffrey Demanes, M.D., Gillian Altieri, C.M.D., David Brandt, M.A., Marie-Claire Barnaba, M.S.N.,-N.P., Lionel Schour, M.D., Pat Skoolisariyaporn, M.S. California Endocurietherapy Cancer Center, Oakland, CA.
Presented Date: Presentation at American Society for Therapeutic Radiology And Oncology (ASTRO) Conference October 2005
| Links to Poster: |
Abstract
Purpose:To report outcome of HDR brachytherapy and EBRT with and without short-term (< 6 month) pre-treatment or concomitant androgen suppression (AS). |
Methods and Materials:Between Sept. 1991 and Dec. 1998, 411 consecutive patients were treated with HDR and EBRT. Median follow up was 7 years (range 5-12 years). Cases were stratified by AS and risk group: 200 AS group I (low 20%, intermediate 48%, high 32%) and 211 no-AS group 2 (low 33%, intermediate 44%, high 23%). General clinical failure(GCF) end points were local or distant failure, PSA >25, or placement or post-treatment androgen suppression. General clinical control (GCC) was the inverse of GCF. SA progression free survival (PSA-PFS) was determined by the ASTRO definition of failure. |
Results:Overall PSA-PFS at 8 years was 85% and by risk group: low 93%, intermediate 86% and high 71%. Overall roup comparison between AS and no-AS revealed no significant difference in GCC (89% vs 89%), PSA-PFS (86% vs 83%), or CSS (96.5% vs 97%). Clinical local control was 99%. Analysis of PSA progression ACCORDING TO RISK GROUP revealed no difference between AS and no-AS despite the higher rate of whole pelvic radiation for the AS group (20% vs. 1.5%) |
Conclusion:Delivery of accelerated HDR brachytherapy is an important outcome determinant. Unlike findings from randomized trials for EBRT alone, results with HDR, stratified by risk group, were not improved by short term AS. |
Back to Top7. High dose rate prostate brachytherapy: the California Endocurietherapy (CET) Method
Author: D. Jeffrey Demanes, M.D.,
Published Date: July 20th, 2000
Medical Journal: Radiotherapy and Oncology, Volume 57, Issue 3, Pages 289-296
Abstract:
Purpose:To describe the rationale, protocol and procedure for the treatment of prostate cancer using high dose rate brachytherapy (HDR-BT) and a non-fixed template technique. |
Methods and Materials:Between July 1991 and December 1998, 491 patients with carcinoma of the prostate were treated using HDR-BT and a non-fixed template technique. AJC stages T1C–T3B, patients with prior transurethral resections of the prostate (TURP) and gland volumes >60 cm3, were included. Flexible cystoscopy, fluoroscopy and transrectal ultrasound (TRUS) were used and 17 flexiguides were inserted through the perineum. Dosimetry was carried out using localization films. Treatment volume was defined at 4–6 mm outside the peripheral catheters. BT consisted of two implants, separated by 1 week, with two fractions given per implant for a total of four HDR fractions. Dose prescription to the treatment volume was 6 Gy (HDR) per fraction, with an additional dose of 0.5 to 0.75 Gy given where required. |
Results:Patients with glands >60 cm3, narrow pubic arches and TURP defects were treated satisfactorily. Symptoms of urinary irritation occurred with variable intensity and abated rapidly 2 weeks after the procedures. There was no high-grade chronic rectal morbidity and most patients reported no rectal symptoms or treatment-related chronic urinary incontinence. |
Conclusion:The non-fixed template technique allowed flexibility in flexiguide placement to encompass large glands (>60 cm3), extracapsular extension and seminal vesicle involvement without the need for additional flexiguides. Also, small pubic arches and TURP defects posed little problem in positioning the flexiguides. This versatility resulted in complete treatment volume coverage of the prostate. |
Home
Treatment Programs
- Prostate Cancer

 Monotherapy Survival Rate
Monotherapy Survival Rate- Breast Cancer
- Vaginal Cancer
- Cervical Cancer
- Endometrial Cancer
- Vulvar cancer
- Head and Neck Cancer
- Lung Cancer
- Esophageal Cancer
- Bile Duct Cancer
- Soft Tissue Sarcoma Cancer
Treatments Statistics
Glossary
Frequently Ask Questions
General Information
Brachytherapy Publications
Cancer Resources & Links
Back to TopGeneral Frequently Asked Questions
1. What is Brachytherapy?
The prefix "brachy" is the Greek word for "short" distance. Brachytherapy is a form of internal radiation treatment where radioactive sources are placed on or into cancer tissues. There are two kinds of brachytherapy. The radiation sources may be inserted either permanently or temporarily. The two most common forms of treatment are low dose rate (LDR) permanent seeds for prostate cancer and high dose rate (HDR) temporary brachytherapy, that can be used for prostate, gynecologic, breast, head and neck, lung, esophageal, bile duct, anorectal, sarcoma, and other cancers.
2. What is high dose rate (HDR) Brachytherapy?
High dose rate (HDR) is a technically advanced form of brachytherapy. A high intensity radiation source is delivered with millimeter precision under computer guidance directly into the tumor killing it from the inside out while avoiding injury to surrounding normal healthy tissue. For a more in depth explanation please visit the understanding HDR Brachytherapy page.
3. How does radiation kill cancer?
Cancer is made of abnormal cells that tend to grow without control. Cancer DNA is more sensitive to radiation than are normal cells, so radiation kills cancer directly or when the cells attempt to multiply while normal tissue in the region is able to repair and recover.
4. What are the advantages of HDR Brachytherapy?
- Short course of treatment compared to other types of radiation treatment (1 week)
- Preservation of organ structure and function
- Fewer side effects
- Excellent coverage of possible microscopic extension of cancer
- Knowledge of radiation dose distribution before treatment is given
- Accuracy and precision of tumor specific radiation dose delivery
- Minimizes areas of radiation overdose (hot spots) or underdose (cold spots)
- Organ motion (target movement) is not a problem for HDR as it is with external beam
| Prostate Specific |
- Effective treatment for cancer recurrence (termed "salvage" therapy)
- No radiation source (seeds) migration into other organs
- No radiation exposure to other persons
| Breast Specific |
- Conserves the breast and yields excellent cosmetic results
- Reduces radiation dose to the heart, lungs, and opposite breast
- Doesn't cause a delay in other treatments such as chemotherapy
For more information on the advantages for specific cancer sites please click on the appropriate link below:
Prostate cancer | Breast Cancer | Gynecologic Cancer | Head & Neck Cancer
Esophageal and Bile Duct Cancer | Lung Cancer | Soft Tissue Sarcoma Cancer
5. How successful is HDR Brachytherapy?
HDR Brachytherapy is effective treatment of local disease in many forms of cancer including prostate, gynecological, breast, head and neck, esophagus, lung, anorectal, bile duct, sarcoma, and other primary cancer or localized metastasis as reported in medical literature. CET's publication on prostate cancer, for example has demonstrated 90% 10-year tumor control. Success rates for other tumors vary according to the type and stage of cancer being treated.
6. How many treatments has CET administered?
As of 10/31/2009, CET has performed 10,217 HDR implants and delivered 21,747 HDR treatments. Please see our treatment statistics for further details.
7. Why is HDR less well known than other forms of cancer treatment?
HDR Brachytherapy is a relatively new form of advance radiation technology. Fewer physicians have been trained to perform HDR procedures compared to seed implants or external beam radiation. Few centers, other than CET have been dedicated to the development of HDR brachytherapy to its full potential. Dr. Demanes has devoted his career to the advancement of brachytherapy and has pioneered the use of HDR and established CET as a center of excellence with specially trained and experienced staff and physicians.
8. Why should I select CET?
- Most experienced HDR center in the country
- First center specializing solely in HDR brachytherapy
- Recognized as HDR experts by colleagues in radiation oncology
- Acknowledged safety record
- Highly trained and experienced physicians and staff
- Long term results published in peer reviewed medical literature
- Quality patient care and follow up
Back to TopAbout Us
-
California Endocurietherapy Cancer Center (CET) is the first brachytherapy only center in the United States.
-
Founded by D Jeffrey Demanes M.D. in 1981.
-
Dedicated solely to High Dose Rate brachytherapy (HDR) since 1991.
-
Most experienced HDR brachytherapy center.
-
A training destination for physicians and residents.
-
HDR treatment protocol development
-
Innovation in high dose rate brachytherapy and equipment design
-
Dedicated to long-term follow-up, outcome studies, and publications in medical journals.
Membership and affiliations
 |
 |
 |
| American Society for Therapeutic Radiology And Oncology Chair - Health Policy and Economics Practice Management Subcommittee, Chair - Regulatory Subcommittee, Member - Health Policy and Economic Committee, Member - Health Policy and Economics Code Development and Valuation Subcommittee, Member - Code Utilization and Application Subcommittee. American Brachytherapy Society Chair - Socioeconomic Committee. American College of Radiation Oncology President - 2005 to 2007 American College of Radiology Fellow - 2007 |
Back to Top
CALIFORNIA ENDOCURIETHERAPY AT UCLA
Division of BrachytherapyDepartment of Radiation Oncology
200 UCLA Medical Plaza, Suite B265
Los Angeles, CA 90095-6951
Tel: 310-206-2510 Fax: 310-794-9795
Hours: Mon-Fri, 8:30AM to 5:00PM Pacific Time
Copyright California Endocurietherapy Medical Corp. All Rights Reserved. www.cetcancercenter.com